
Elizabeth Wood and Sarah Flynn South of England Cochlear Implant Centre, Institute of Sound and Vibration Research, University of Southampton, Southampton SO17 1BJ
Back to index of articlesFM radio aid systems have been standard equipment for many years for children with hearing loss in educational settings where listening conditions can be poor. The primary benefit is the improvement of signal level and signal to noise ratio for the listener and benefits of the use of the FM microphone are typically in the range of 15-20dB (Ross 1992). As a significant number of children with cochlear implants are now being educated in mainstream schools, the successful use of an FM radio aid will direct rehabilitation at the hearing deficit rather than overcoming the poor listening environment.
There have been problems of range and interference, associated with combining an FM aid with a cochlear implant processor. Both systems operate on radio frequencies and there can be some overlap of frequency harmonics. (UK FM systems operate in the 173-175 MHz band and speech processors between 2.5MHz and 49MHz depending on the individual system). As an FM radio aid transmits much less power than a cochlear implant system it is more susceptible to interference. It was found that some of the radio frequency energy generated by the speech processor was present on the FM interface cable. As this was also the aerial of the receiver the potential for interference was increased resulting in poor range, and poor sound quality (Boyle et al 1997,Wei et al, Popplestone 1998). Early work reported by the South of England Cochlear Implant Centre established that although systems were compatible there were problems of interference for most users. Many of these technical problems have been addressed and research studies have improved our understanding.
Research rationale and test materials
Subjects used for our research trials have been older children and adults, all who have used their cochlear implant processor for more than 9 months and who are able to report on sound quality. We have used word discrimination testing in pink noise and have tested at distances up to 10 metres to simulate classroom conditions. These standard conditions have enabled us to compare different processor and radio aid combinations. The IHR-McCormick Automated Toy Test (ATT) (McCormick 1977) was used. This is a speech discrimination task with words within the child's vocabulary, so that the scores reflect speech perception errors, with no influence of language. The test uses seven pairs of toys matched with a similar vowel or diphthong, but differing consonants (e.g. cup/duck, fork/horse). The computerised version is delivered through a PC with software running Windows 95. The test uses an adaptive technique to record a speech discrimination level in dBA, at which the subject scores 71% correct.
Early FM Studies
The benefit of FM study (Wood, Flynn & Eyles 2000) compared speech discrimination in quiet and in noise, with and without an FM radio aid. Nucleus Spectra and Sprint Speech Processors were used. The radio aids used were the Connevans CRM 220 and the Phonic Ear 475. The FM radio aids were set up in accordance with the cochlear implant manufacturers guidelines, but when used the sensitivity of the speech processor was not reduced. The speech was delivered from the loudspeaker at 1 metre, and the FM transmitter was placed 20cm from the speaker. All children benefited from using the FM system in noise, the mean benefit for using FM in noise was 15dB and in quiet was 7dB, probably because of reduced distance between the speaker's voice and the microphone. There was considerable individual variation
The second study evaluated speech discrimination over distance (Flynn Wood and Eyles 2000). The ATT was used so the results could be directly compared. Subjects listened with one of five radio aids (Phonic Ear, Solaris, Microvox, Sennheiser and Connevans 220) at three distances (1, 3 and 10 metres). Subjects were asked to give subjective feedback about sound quality at each distance and rate the sound as clear, sharp, muffled and whether there was any hissing, buzzing or echo. The sound quality was reported as good at all distances with all radio aids with a mean improvement at 1 and 3 metres of 14 dB, and at 10 metres of 10 dB. Patient feedback was valuable. We concluded that all the radio aids had a good transmitting range and gave good quality sound.
Use of FM in the UK
The third piece of research was a survey that was sent to all cochlear implant centres in the UK (Wood and Flynn 2000). We received data on 1241 children who had received a cochlear implant. 33% (N=411) of these children used FM systems and of these 54% were using the Connevans 220. A small number (N=13) were using FM soundfield systems. 97% of children fitted with FM systems were using Nucleus cochlear implants, but at that time the connecting leads were not available for the Medel and Advanced Bionics speech processors.
Appropriate fitting time
Staff at Implant Centres is frequently asked how soon can a child be fitted with an FM system, especially if the child or young adult was a previously good user of hearing aids with a radio aid. There are three important issues to consider.
Firstly, it is very important that the user has a stable map, and this can take up to a year post implant, especially with young children.
Secondly, the individual must be a reliable user of their implant and be able to report a fault, including any extraneous noises or no sound.
Thirdly, the local professionals need to be fully aware of the implications
- the need for initial fitting at the Implant Centre
- the correct wearing position
- the need to be aware of potential sources of interference so they can advise the schools. In the survey we found that 50% of the cochlear implant centres in the UK fitted radio aids between 12 and 17 months post implant.
Soundfield systems are becoming more commonly used in schools, either a classroom soundfield amplification system, or a portable desktop system. A classroom system will benefit all children and the class teacher but will only provide an improvement in signal to noise ratio of approximately 10 dB.
We received reports from cochlear implant users in schools where a personal FM radio aid was used in soundfield treated classrooms and halls which suggested that the quality of the combined signal was not optimal. A small study involved recording a short speech passage played though a Sprint speech processor, in soundfield treated areas, with and without a radio aid. Sound quality was rated in the different settings and we found that the ratings were poorest in the halls, which had not been acoustically treated before the soundfield system had been installed. The implant wearers expressed a preference for wearing the radio aid alone in these halls, but were happier using the two systems together in rooms which had good acoustics (Wood et al 2002).
Inglehart FN (2003) reported that optimal speech perception is not met for students with cochlear implants in noisy, reverberant classrooms by the use of soundfield systems alone; acoustics also need improvement. The new Building Bulletin 93 (BB93) 'Acoustic Design of Schools' 2003, should address this issue. However, there may still be instances where the soundfield treatment is not optimal so cochlear implant users are not benefiting from using the combined systems.
Results with the ESPrit 3G
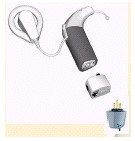
When connecting an ESPrit 3G to a radio aid an audio accessory adaptor is plugged in at the base of the 3G, and the FM cable is plugged into the adaptor.

Cochlear have developed a MicroLink adaptor to use with the Phonak MLx and MLxS MicroLink receivers. The picture below shows the ESPrit 3G with the adaptor and MLxS receiver.
Our first study (Wood Flynn Greenham & Eyles 2003) evaluated the use of the Nucleus ESPrit 3G ear level speech processor with the Phonak MicroLink MLx, the Connevans 220, Connevans Genie, and the Phonic Ear Solaris. Subjects reported problems with the clarity of the FM signal with the MicroLink MLx. A need was identified for a change to be made to the programming parameters of the ESPrit 3G speech processor. The monitor earphones should NOT be enabled on the map that is to be used for FM and accessories.
The results of the second study (Wood Flynn Greenham 2003) indicated that the MicroLink MLx, Solaris and Connevans Genie performed well with the ESPrit 3G in noise, and over distance when sound quality was rated at >83% for all three systems. However 6/10 subjects preferred the Genie or Solaris due to the louder sound and the word discrimination results were significantly better at 3 and 10 metres with the Genie compared with the MLx.
Further research questions were posed as the Handymic transmitter had been used in the directional setting and had this had an effect on the results? Also would the MLx be more acceptable if there was a higher gain option? Preliminary results suggest that the omni microphone setting is to be recommended for the Handymic and the newer Campus S transmitter. The MLx has a gain setting of +7. The new Phonak MicroLink receiver, the MLxS, has factory set variable gain options from +10 to +24. Our current research is repeating the word discrimination task in noise and over distance with the MicroLink MLxS at gain settings of +10, +16 and +20. This research is not yet fully completed but results suggest that the MLxS with higher gain settings does give improvements for listening, but one gain setting is unlikely to suit all cochlear implant users. The results also suggested that gains of greater than +16 resulted in less comfortable listening levels for a substantial proportion of subjects. The gain setting for the MLxS is, at present, set by the manufacturers (Phonak) but discussions are taking place to establish if this will be the preferred method for the future. Full results will be reported on this summer.
Fitting guidance and procedure
As education services provide the radio aid, initial discussions should take place with a member from the cochlear implant team to establish that the child is ready and willing to accept a second piece of equipment. The implant user's map must be stable and the wearer must be able to report on sound quality. A particular transmission frequency may be recommended to reduce the possibility of interference e.g. for the Sprint and ESPrit 3G this will be frequencies 0,1,2,3 for the Genie (or equivalent for other radio aids), but for the Esprit 22 frequencies 9,10,11 for the Genie (or equivalent for other radio aids).
At our centre we have successfully fitted 75/132 (57%) of children with radio aids as shown in the chart below. The majority of the children who are not using a radio aid are those who are not 'ready' yet.
The first fitting generally takes place at about one year post implant and we recommend that this take place at the cochlear implant centre when issues can be discussed. We will provide the correct FM lead, advise on wearing position and set the radio aid up so that the output is compatible with that from the cochlear implant. One of the maps in the ESPrit 3G speech processor will be recommended for use with the radio aid and accessories, with the monitor earphones NOT enabled.
Procedure for fitting a radio aid with a Nucleus or Med-el cochlear implant processor
Check the radio aid, set any internal switches, listen to it and set it at an appropriate volume*
Check the speech processor is functioning optimally
Select the appropriate map
Start with the speech processor and FM system switched off
Use the appropriate connector to attach the correct end of the FM cable to the speech processor. This may be:
- An audio shoe for the Esprit 22
- An audio adaptor for the ESPrit 3G
- The top socket of the Sprint or Spectra
- The audio socket for the Medel Cis-Pro+
- Under the hinged part of the Medel Tempo+
Switch on the radio aid transmitter
Switch on the radio aid receiver*
Switch on the speech processor
Validate the FM receiver setting by using a speech discrimination task and readjust if necessary (in the clinic we will use the McCormick ATT, but in the classroom the LING sounds test can be used).
We issue an FM booklet that details the settings, speech processor map number and location, recommended sensitivity and instructions for the correct sequence for connecting the systems. Advice is also given about interference. It is important that a muting switch is always used (e.g. with Connevans Genie or Connevans 220 transmitter) as if a transmitter is switched off but the child has the receiver switched on, there is a strong likelihood of the user hearing a hissing noise.
*Appropriate volume setting for the radio aid receiver
Through our validation procedure we have ascertained the volume settings for different radio aids and speech processors. These will vary slightly for individual children so it is not possible to state definitive figures. For example, most children will use the Connevans Genie receiver on volume 4-5 with an ear level ESPrit 22, 24 or 3G speech processor but we have examples of adults who have helped us with our research, and children in school who like the volume to be between 1-2. The volume setting will be higher when using a Sprint speech processor with the Genie (usually about volume 6), and the Solaris receiver usually needs to be set at almost maximum for the Sprint but at about volume 5 with an ear level ESPrit 22, 24 or 3G. When initially setting the volume for a first fitting we will be cautious and turn it up gradually, watching the child all the time.
We do not recommend that the sensitivity of the speech processor be reduced. The ear level microphone on the user's speech processor needs to be active so they can hear their peers easily, and if appropriate, the voice of the learning support assistant who may be sitting next to them.
Checking the systems
Monitor earphones can be used to check the combined signal for the Sprint speech processor, but as this is not possible for the ESPrit 3G, the ESPrit 22 or the Medel Tempo+, it is advisable to seek feedback from the user.
The sensitivity on the child's speech processor can be turned down to 0, and then with the child at a distance, the teacher can speak into the transmitter and the child can be asked to listen and report on the FM alone signal.
Other tips are to switch an ESPrit processor off and on again, check that the accessory adaptor is being used and to check both the adaptor and the FM lead are fully connected. The MicroLink MLx and MLxS receivers should be switched to the 2-dot position and the cochlear adaptor should be switched to FM+mic position. The HandyMic and Campus S transmitter should be switched to the omni mic position.
Conclusions
The increasing number of children who are successfully using FM radio aids with their cochlear implants encourages us. At the implant centre we are becoming more aware of potential pitfalls and are able to offer suggestions to colleagues to enhance their skills and understanding. The children will be better able to access the curriculum by improving their listening conditions. We have worked with cochlear implant manufacturers and radio aid manufacturers and ideas and recommendations have been implemented. We feel pleased that the children we have fitted are generally giving us good feedback and like to wear their radio aids in the classroom.
References
Boyle P et al 1997 Compatibility of the Clarion cochlear implant with the Connevans CRM-220 ENT Journal Vol. 76 no 6
FlynnSL Wood EJ Eyles JA. 2000 Speech Discrimination with FM Radio Aid Systems and cochlear implant users: Results over distance. Poster presentation 5th European Symposium on Paediatric Cochlear Implantation.
Inglehart FN 2003 Oral presentation 9th Symposium Cochlear Implantation in Children
McCormick B 1997 The Toy Discrimination Test Public Health London 91
Popplestone J 1998 The use of FM radio microphone systems with cochlear implants Connevans Ltd
Ross M (Ed) 1992 FM auditory Training Systems Timonium, MD York Press, Inc
Wei J et al Compatibility of the S-series cochlear implant with FM hearing aid systems Clarion by Advanced Bionics publication
Wood EJ Flynn SL Eyles JA 2000 The benefit of using an FM radio aid system with cochlear implant users Poster presentation 6th International Cochlear Implant Conference.
Flynn SLWood EJ Eyles JA 2000 Speech discrimination with FM radio aid systems and cochlear implant users: Results over distance. Poster presentation 5th European Symposium on Paaediatric Cochlear Implantation
Wood EJ and Flynn SL 2000 A survey investigating the use of Fm Radio Aid Systems with cochlear implant users in the UK. Oral presentation 19th Congress on Education of the Deaf
Wood EJ Harriott MM Shann J 2002 An investigation into the use of an FM radio aid in a classroom/hall with a soundfield system. Oral presentation 6th European Symposium on Paediatric Cochlear Implantation.
Wood EJ Flynn SL Eyles JA Greenham P 2003 The benefit of using an FM radio aid over distance and in noise with the Nucleus ESPrit 3G speech processor. Poster presentation 9th Symposium Cochlear Implantation in Children
Wood EJ Flynn SL Greenham P 2003 The benefit of using an FM radio aid over distance and in noise with the ESPrit 3G speech processor. Poster presentation ACCESS Conference
We would like to acknowledge our co-workers and the help from the radio aid manufacturers for the loan of the radio systems.